Arthroscopy is a surgical technique that involves the introduction of a small circular lens (2.0 to 6.0 mm in diameter) into a joint for the purpose of inspection and possible treatment. The arthroscope is an elongated tube possessing a series of lenses that allow for the magnification of structures within the joint. A camera is affixed to end of the arthroscope so that joint images can be projected onto a television monitor. Small incisions (one-quarter inch or less) are placed strategically around the joint to allow for the introduction of the arthroscope, as well as other pieces of equipment needed for the precise correction of joint injury.
Arthoscopy vs. Arthrotomy (Open Technique)
Arthroscopy offers several advantages over classical "open joint" (arthrotomy) techniques. First, arthroscopic evaluation and treatment only requires small incisions in the joint capsule, limiting the degree of scarring and trauma associated with surgery. Second, the environment within the joint is more easily inspected by virtue of the magnification provided by the arthroscope. Third, removal of damaged joint tissue or scarring is achieved in a more precise manner as a consequence of the very fine, specially designed equipment. Fourth, the joint is continuously bathed in physiological fluids providing a healthier environment during surgery. This is in contrast to open joint techniques where the cartilage surface is exposed to air within the operating room, potentially compromising its viability. Unfortunately, situations do arise when the joint needs to be opened in order to achieve the objectives of the surgical procedure. For example, certain cartilage injuries within the ankle joint may be located in areas where arthroscopic visualization is poor, or access to the lesion with available equipment is nearly impossible. In these cases, even though an arthrotomy was necessary due to inaccessibility, the arthroscope is invaluable in specifically identifying the location, and extent of the problem.
Ankle and Subtalar Anatomy
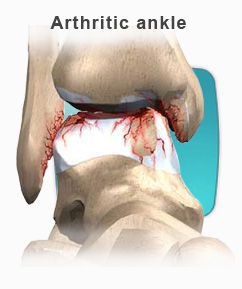
The ankle joint is comprised of three bones, the tibia (inner ankle and leg bone), the fibula(outer ankle and leg bone), and the talus (odd shaped, lower ankle bone). The ankle joint space is found between the talus and the tibia, as well as between the talus and the fibula. A large majority of the articular surface of the talus is in contact with the cartilage surface of the tibia. These two surfaces are slightly dome shaped from front to back. The ankle joint allows the foot to mobilize up (dorsiflexion) and down (plantarflexion). There are three major ligaments associated with the outer part of the ankle joint: the Anterior Talofibular, Calcaneofibular, and Posterior Talofibular ligaments. There is one major ligament with several bands associated with the inner part of the joint: the Deltoid ligament. Together these ligaments guide motion and provide stability to the ankle joint.
The lower ankle joint or subtalar joint (below the talus) exists between the talus and the heel bone (calcaneus). The subtalar joint is actually made up of two anatomically distinct joints. These two joints are separated by a void or space, which houses the two major ligamentous stabilizers of the subtalar joint: the Interosseous Talocalcaneal and Cervical Ligaments. Further stability is afforded to the subtalar joint by one of the three lateral ankle ligaments (Calcaneofibular Ligament), and several bands of the main inner or medial ankle ligament (Deltoid Ligament). The subtalar joint allows the foot to pronate and supinate. Supination of the subtalar joint involves movement of the foot in an inward direction, so that the sole of the foot faces the opposite limb. Pronation of the subtalar joint involves movement of the foot in an outward direction, allowing the sole to face away from the opposite limb.
Rearfoot and Ankle Inversion Injuries: Mechanism of Injury
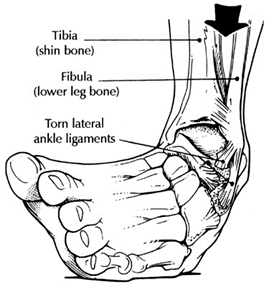
During a common ankle sprain, the foot is forcibly rotated inward toward the opposite leg. The inward movement of the foot is a motion well accommodated by the lower ankle joint (subtalar joint), but not by the upper or true ankle joint. Ultimately, the lower ankle joint comes to the end of its available inward motion, and stops rather abruptly (the lower ankle joint can be injured at this point). Continued inward movement of the foot forces the ankle joint in a direction it is not designed to accommodate. The lower ankle bone or talus is thus forcibly directed inward, partially dislocating the talus out from under the tibia and fibula. It is not uncommon for the outer ankle ligaments to be partially or completely torn, resulting in joint instability. Furthermore, the adjacent joint surfaces can collide or impinge during the injury, resulting in disruption of the cartilage surface.
Arthroscopy: Indications for usage
Arthroscopy is an effective tool for the evaluation and management of pain localized to the ankle or lower ankle (subtalar) joints. Following an ankle sprain, ligamentous scarring can occur within various regions of the ankle or subtalar joints. Arthroscopy allows direct visualization and precise removal of scar tissue with minimal joint trauma. Generally, two to four portals or incisions are required for ankle arthroscopy, and two or three for subtalar arthroscopy. Loose fragments of bone, cartilage or ligament can be identified and removed through the small portals in the joint capsule. Occasionally, small accessory incisions may be necessary to remove larger fragments of tissue found within the joint. Regions of the joint surface that have been injured will commonly display an obvious defect or a loose flap of cartilage that has been delaminated from the underlying bone. Not infrequently, the joint surface will appear normal; however, gentle probing will reveal an area of softness compared to surrounding cartilage. These soft areas are regions of cartilage injury and will require removal of the damaged cartilage. In some cases, physicians are drilling small holes through these soft zones in order to promote re-adhesion of the cartilage. In areas where there is an obvious defect in the cartilage surface, the damaged cartilage is removed down to normal cartilage. Following the removal of damaged cartilage, the exposed underlying bone is drilled repetitively to facilitate bleeding into the base of the injured area. The blood will form a clot across the full dimensions of the defect. Over time the blood clot is converted to cartilage. The repair cartilage is not of the same quality as was originally present; however, the repair cartilage re-establishes near normal surface-to-surface contact. In some cases, small plugs of normal cartilage and bone can be removed from one location within the ankle joint, and placed into an area of cartilage injury. Unfortunately, transport of cartilage within the ankle joint necessitates an open joint technique and cannot be performed arthroscopically.
Arthroscopy has also been useful in assisting with the repair of fractures that involve the surfaces of the ankle joint (Pilon fractures or talar fractures). In these cases, the arthroscope is used to visualize the fractured joint surface as it is repaired to assure accurate realignment. Arthroscopy has also been used to visualize the joint during removal of the articular cartilage prior to fusion of the ankle joint.
Conditions Where Arthroscopy may not be Useful
Unfortunately, arthroscopy is not helpful in certain types of joint injury. If a cartilage lesion is located in the central or back portion of the joint, many times the lesion cannot be accessed with the arthroscope. In these cases, the tibia or inner ankle bone must be cut in order to allow inspection and treatment of the lesion. Ankle fusions cannot be performed arthroscopically if a large degree of malalignment exists within the ankle joint itself. In these cases, the joint must be opened and the joint surface remodeled to reduce the deformity. Although some surgeons are repairing single ligament tears through the arthroscope, this has not gained universal acceptance. Significant joint instability associated with multi-ligament injury requires open joint repair or reconstruction techniques.
Arthroscopic Surgery of the Ankle and Subtalar Joints
Arthroscopic surgery of either the ankle or subtalar joints is generally considered an outpatient (same day) surgical procedure. Pre-operatively or intra-operatively, patients are usually given antibiotics to reduce the risk of infection. The surgery can be performed under either general or spinal anesthesia. Arthroscopy can also be performed under local anesthesia with IV sedation. The latter procedure requires the anesthesiologist to use a local anesthetic to block the large nerve behind the knee joint (main nerve block). The surgeon will further supplement the main block with local anesthetic infiltrated just above the ankle joint. The patient is then kept in a twilight sleep with medications infiltrated through the IV by the anesthesiologist. Post-operatively, the ankle is lightly bandaged. The patient may be placed in a removable cast boot or splint to keep the ankle at 90 degrees to the leg; however, gentle range of motion is recommended on a regular basis after surgery. Following surgery, patients are usually non-weight bearing for 7-14 days, and then are allowed to weight bear as tolerated. If a large cartilage lesion was either drilled or cleaned out, patients will remain non-weight bearing up to 4 weeks. The actual duration of non-weight bearing will depend on the extent of the injury and the type of treatment rendered. It is not uncommon for patients to undergo physical therapy after surgery, especially if they had a prolonged period of pain and disuse prior to surgery.
Risks and Complications Associated with Ankle or Subtalar Arthroscopy
Like any other surgical procedure, arthroscopy has certain inherent risks and complications. In the author's experience, these have been uncommon. The literature sites injuries to the superficial nerves as the most common complication after ankle arthroscopy. Most of these nerve related injuries result in tingling, numbness, or occasionally burning sensations across the outer part of the ankle onto the top of the foot. Most of these sensations resolve over a period of 3-5 months. Obviously, more significant nerve related injuries have been reported, but they are uncommon. There is the risk of infection; this complication is rarely seen with appropriate antibiotic prophylaxis prior to surgery and sterile technique during surgery
Conclusions
Arthroscopy of the ankle or subtalar joints has proven to be a valuable tool for treating various injuries to these unique joints. The degree of joint and soft tissue trauma associated with arthroscopy is no doubt less than open joint techniques, resulting in somewhat faster healing times. Immediate return to walking and sports is not usually recommended. The joint can be often sore and swollen for several weeks after surgery. Aggressive and rapid return to activity can result in a more prolonged recovery time. Listen to physician instructions and follow carefully.




 Blisters form as a result of heat, moisture and friction. Blisters can also form as a result of fungal infections of the skin, allergic reactions or burns. If a patient has diabetes, they should be evaluated by a doctor in a timely fashion. Generally, a person will recognize a burn by association with a specific painful event. People with diabetes may not be able recognize the painful event due to a condition called neuropathy. A doctor should attend to burns. Blisters are due to fungal infection of the skin or to allergic reactions, which will generally occur in clusters and be smaller than blisters caused by friction. They will also often occur in areas of the foot, which are free from friction forces.
Blisters form as a result of heat, moisture and friction. Blisters can also form as a result of fungal infections of the skin, allergic reactions or burns. If a patient has diabetes, they should be evaluated by a doctor in a timely fashion. Generally, a person will recognize a burn by association with a specific painful event. People with diabetes may not be able recognize the painful event due to a condition called neuropathy. A doctor should attend to burns. Blisters are due to fungal infection of the skin or to allergic reactions, which will generally occur in clusters and be smaller than blisters caused by friction. They will also often occur in areas of the foot, which are free from friction forces. Blisters should be drained leaving the cover of the blister in tact. The area should be protected with a non-stick bandage with mild compression. Ice to "hot spots" can be soothing and reduce the thermal damage to the surrounding area. "Double socking" can prevent blisters associated with athletics. Wearing two pair of socks allows the friction to be absorbed between the socks reducing friction to the skin. A sock has been developed that helps to reduce friction and blistering called the Thro-lo sock. It is useful for athletics and for diabetic patients. They are widely available in athletic shoe and apparel stores. Skin protectant sprays and adhesive gel pads are also available.
Blisters should be drained leaving the cover of the blister in tact. The area should be protected with a non-stick bandage with mild compression. Ice to "hot spots" can be soothing and reduce the thermal damage to the surrounding area. "Double socking" can prevent blisters associated with athletics. Wearing two pair of socks allows the friction to be absorbed between the socks reducing friction to the skin. A sock has been developed that helps to reduce friction and blistering called the Thro-lo sock. It is useful for athletics and for diabetic patients. They are widely available in athletic shoe and apparel stores. Skin protectant sprays and adhesive gel pads are also available. Athlete's foot is caused by a fungal infection of the skin on the foot. The majority of these infections are caused by one of three fungal agents called dermatophytes. Athlete's foot is by far the most common fungal infection of the skin. The infection can be either acute or chronic. The recurrent form of the disease is often associated with fungal-infected toenails. The acute form of the infection most often presents with moist, scaling between the toes with occasional small blisters and/or fissures. As the blistering breaks, the infection spreads and can involve large areas of the skin on the foot. The burning and itching that accompany the blisters may cause great discomfort that can be relieved by opening and draining the blisters or applying cool water compresses. The infection can also occur as isolated circular lesions on the bottom or top of the foot. As the skin breaks down from the fungal infection, a secondary bacterial infection can ensue.
Athlete's foot is caused by a fungal infection of the skin on the foot. The majority of these infections are caused by one of three fungal agents called dermatophytes. Athlete's foot is by far the most common fungal infection of the skin. The infection can be either acute or chronic. The recurrent form of the disease is often associated with fungal-infected toenails. The acute form of the infection most often presents with moist, scaling between the toes with occasional small blisters and/or fissures. As the blistering breaks, the infection spreads and can involve large areas of the skin on the foot. The burning and itching that accompany the blisters may cause great discomfort that can be relieved by opening and draining the blisters or applying cool water compresses. The infection can also occur as isolated circular lesions on the bottom or top of the foot. As the skin breaks down from the fungal infection, a secondary bacterial infection can ensue. The diagnosis of tenia pedis is generally made based upon the clinical presentation. A definitive diagnosis is made by taking a scraping of the skin and culturing it. It may take up to three weeks for the culture to grow the fungus. In some instances the culture may present a false negative result because the skin scraping was inadequate. Some doctors may perform a KOH prep of a skin scraping. This is examined under a microscope and may reveal elements that can make the diagnosis.
The diagnosis of tenia pedis is generally made based upon the clinical presentation. A definitive diagnosis is made by taking a scraping of the skin and culturing it. It may take up to three weeks for the culture to grow the fungus. In some instances the culture may present a false negative result because the skin scraping was inadequate. Some doctors may perform a KOH prep of a skin scraping. This is examined under a microscope and may reveal elements that can make the diagnosis.
 Chronic ankle instability is the recurring “rolling” or “giving away” of the outer side of the ankle. The ligaments on the lateral side of the ankle may become weakened over time and after repeated ankle sprains. Typically the “rolling” or “giving away” occurs when walking or being active. This is a common occurrence with athletes. However, this can even happen when simply standing.
Chronic ankle instability is the recurring “rolling” or “giving away” of the outer side of the ankle. The ligaments on the lateral side of the ankle may become weakened over time and after repeated ankle sprains. Typically the “rolling” or “giving away” occurs when walking or being active. This is a common occurrence with athletes. However, this can even happen when simply standing.