Our Issaquah clinic is kid friendly! We see a large number of children from the Seattle area and beyond. There are a variety of problems that can affect their feet.
Arch Problems and Walking Problems
Many children start life off with low arches. We all start out life with quite a bit of "baby fat." It's surprising, but this is even in the foot and especially the instep. This makes it difficult to tell if the young child has a normal arch or not. The problem is, that sometimes they don't have a normal arch. Even in these cases, sometimes the parents are told that they will outgrow this low arch or flatfoot. However, many children do not outgrow these problems and they become lifelong challenges. We evaluate and treat a number of these different arch and walking concerns.
Heel Pain
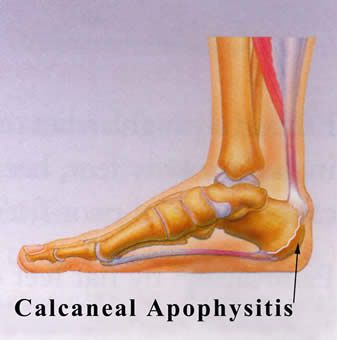
Many of our pediatric patients have pain in their heels. This makes it difficult to do the sports they like. We have developed treatments that can eliminate this heel pain rapidly. A common cause of this heel pain is irritation to the growth plate in the heel bone (calcaneal apophysitisor Sever's Disease). Other possible causes include Achilles tendonitis and plantar fasciitis.
Growing Pains
Children may complain of pain in their legs during or after activity or sports. Often, this is not really growing pains but rather leg muscle pain and fatigue. These muscles support and control foot function. In adults these can be part of the shinsplint syndrome. Children can get a variation of this. Our clinic has very effective treatments for this condition.
Children's Sports Injuries
We also see and treat foot and ankle injuries. So many kids are doing multiple sports. This is great exercise, but it does put an extra work load on the legs and feet. This can cause problems and injuries ranging from a simple sprain or tendonitis to a fracture that is either a typical fracture or a growth plate type of injury to the bone. Each sport seems to require slightly different treatment considerations. Some of these different sports include soccer, football, basketball, lacrosse, baseball, gymnastics, dance and ballet, track and field, martial arts and volleyball.
Plantar Warts
These are warts on the bottom of the feet. Compared to adults, children are often barefoot, which makes them more vulnerable to these plantar warts. The virus that causes these warts only live in human skin and they can be contagious. These warts can be painful and often are much deeper than expected. What you see on the skin is often just "the tip of the iceberg." Many medical clinics treat all warts with a liquid nitrogen freezing technique; this is often very painful and causes many children to be apprehensive about treatment for plantar warts. However, we have found a number of treatments that are very effective and often do not have any associated pain. Our office has become a treatment center for resistant plantar warts. We work with many of the local pediatricians and family practice clinics to treat these problems.
Ingrown Toenails
Adolescent boys in particular get ingrown toenails. They are growing so fast that their shoes can become snug fitting before they get replaced. This shoe pressure is often a causative factor in ingrown toenails.
For children, we use a combination of topical anesthetic -- ethyl chloride (cold spray), and gentle electrical stimulation. The patient controls electrical stimulation themselves to help keep the nerves "busy." Then, the local anesthetic injection is administered. Our younger patients benefit from this special technique. They are often very apprehensive about an injection, but with our techniques, the patient and their parents are usually pleasantly surprised at how well they do.